
Contents
Anion Gap Metabolic
Hello Guys.. How are you ? Hope all of you are well. Today i will talk about Anion Gap Metabolic. If you are interested to know about Anion Gap Metabolic must read this article.
Definition
The anion gap (AG) is a measure of acid-base balance. Your body maintains balance by holding onto or releasing carbon dioxide through the lungs (acid) or bicarbonate through the kidneys (base). Cations are positive (base) and anions are negative (acid). The anion gap is the difference between the number of cations versus anions. An anion gap can be high, normal, or low (rare). A high anion gap indicates that the presence of more anions than cations, or acidosis. When bicarbonate is used up to correct the acid-base balance, the gap widens (Kraut and Madias, 2007). Normal anion gap metabolic acidosis is also known as hyperchloremic acidosis because the kidneys reabsorb chloride instead of reabsorbing bicarbonate.
The signs of metabolic acidosis
If you have metabolic acidosis, there may not be any signs or symptoms.
Metabolic acidosis of Common signs and symptoms of including as :
- Accelerated heartbeat (tachycardia).
- Confusion or dizziness.
- Feeling very tired (fatigue).
- Loss of appetite.
- Headache.
- Rapid breathing or long, deep breathing.
- Nausea and vomiting.
- Feeling weak.
- Breath that smells sweet or fruity.
Severe cases of metabolic acidosis can cause death.
Causes
Expanded Causes (HARDUP)
- Hyperchloraemia
- Acetazolamide, Addison’s disease
- Renal tubular acidosis
- Diarrhoea, ileostomies, fistulae
- Ureteroenterostomies
- Pancreatoenterostomies
or USEDCRAP
- Ureteroenterostomies
- Small bowel fistula
- Excess Chloride
- Diarrhoea
- Carbonic anhydrase inhibitors
- Renal tubular acidosis
- Addisson’s disease
- Pancreatoenterostomies
CHLORIDE GAIN/BICARBONATE LOSS
- loss of bicarbonate with chloride replacement -> hyperchloraemic acidosis
Loss of base via the bowel
- secretions into the large and small bowel are mostly alkaline with a bicarbonate level higher than that in plasma.
- some typical at risk clinical situations are:
- severe diarrhoea
- villous adenoma
- external drainage of pancreatic or biliary secretions (eg fistulas)
- losses via NG tubes
- urinary diversions
- chronic laxative abuse
- administration of acidifying salts
- chronic laxative abuse
- administration of acidifying salts
Loss of base via the kidney
- RTA type 1, 2 and 4
- see Renal Tubular Acidosis
Gain of mineral acid
- eg HCl infusion
- this should be easily established by history
ACETAZOLAMIDE THERAPY
- normally 85% of filtered bicarbonate is reabsorbed in the proximal tubule and the remaining 15% is reabsorbed in the rest of the tubule
- in patients receiving acetazolamide (or other carbonic anhydrase inhibitors), proximal reabsorption of bicarbonate is decreased resulting in increased distal delivery and HCO3- appears in urine
- this results in a hyperchloraemic metabolic acidosis and is essentially a form of proximal renal tubular acidosis but is usually not classified as such.
GI LOSS
- see HCO3 loss above
EXTRAS
Recovery phase of DKA
- hyperchloraemic metabolic acidosis commonly develops during therapy of diabetic ketoacidosis with normal saline
Oral ingestion of Acidifying Salts
- oral administration of CaCl2 or NH4Cl is equivalent to giving an acid load
- both of these salts are used in acid loading tests for the diagnosis of renal tubular acidosis
- CaCl2 reacts with bicarbonate in the small bowel resulting in the production of insoluble CaCO3 and H+
- the hepatic metabolism of NH4+ to urea results in an equivalent production of H+
Anion Gap Acidosis Mnemonics
Here are some helpful ways to remember the causes of high anion gap acidosis.
The most common mnemonics are:
- KUSMALE
- Ketoacidosis
- Uremia
- Salicylate poisoning
- Methanol
- Aldehyde
- Lactate
- Ethylene glycol
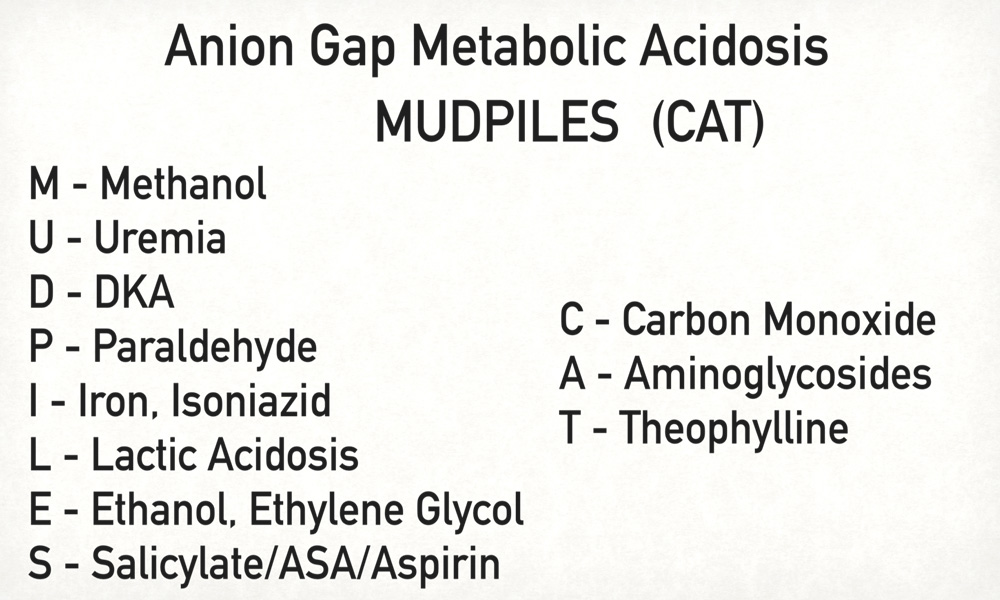
- MUD PILES
- Methanol
- Uremia
- Diabetes
- Paraldehyde
- Iron/Isoniazid
- Lactate
- Ethylene glycol
- Salicylate
A newer mnemonic takes into account the new organic anion gap generating acids and precursors that have been recognized in recent years and replaces paraldehyde which has become exceedingly rare (Mehta, Emmett & Emmett, 2008).
- GOLD MARK
- Glycols
- Oxoproline
- L-lactate
- D-lactate
- Methanol
- Aspirin
- Renal failure
- Ketoacidosis
How do you fix metabolic acidosis?
Once your healthcare provider determines they can recommend an appropriate treatment plan what’s causing metabolic acidosis . Some treatments include:
- Sodium citrate if you have kidney disease or kidney failure.
- Fluids delivered through a vein in your arm (IV fluids).
- IV sodium bicarbonate, which helps balance the acids in your blood.
- Insulin if you have diabetes-related acidosis.
- Removing toxic substances from your blood, including aspirin, methanol (a substance in adhesives, paints and varnishes) or ethylene glycol (a substance in antifreeze).
Treatment
You treat metabolic acidosis by treating what’s causing it. If you don’t restore it can affect your bones, muscles, and kidneys the balance . In severe cases, it can cause shock or death. DKA can put you in a coma.
The earlier you’re treated, the better. Common treatments include:
- Detoxification, if you have drug or alcohol poisoning
- Insulin, if you have DKA
- IV fluids, given by needle through a vein in your arm
- Sodium bicarbonate, by IV
Prevention
There are things you can do to lessen the chance of it happening, You can’t always prevent metabolic acidosis.
Drink plenty of water and non-alcoholic fluids. Your pee should be clear or pale yellow.
Limit alcohol. It can increase acid buildup. It can also dehydrate you.
Manage your diabetes, if you have it.
Follow directions when you take your medications.
FAQs list
1. How to calculate Anion Gap?
Answer : According to your lab (Kraut and Madias, 2007) , The normal value for the serum anion gap is approximately three to 10 mEq/L (averaging six mEq/L) .
2. What are Causes of Anion Gap Acisosis?
Answer : High anion gap acidosis may be caused by:
- ketoacidosis
- lactic acidosis
- renal failure
- toxic ingestions
Normal anion gap acidosis may be caused by:
- gastrointestinal or renal bicarbonate losses
- impaired renal excretion
3. How do you diagnose metabolic acidosis?
Answer : The diagnosis is made by evaluating serum electrolytes and ABGs. A low serum HCO3– and a pH of less than 7.40 upon ABG analysis confirm metabolic acidosis.
4. What infusion corrects metabolic acidosis?
Answer : Sodium bicarbonate should be dispensed as an infusion over several hours.
5. What infusion corrects metabolic acidosis?
Answer : Sodium bicarbonate should be dispensed as an infusion over several hours.
6. What type of anion gap signals acidosis?
Answer : An increase in the anion gap is a sign of metabolic acidosis.
7.What elements impact the anion gap?
Answer : Changes in unmeasured ions have an impact on the anion gap. Due to the metabolism of ketones, there is a rise in keto acids in uncontrolled diabetes. Metabolic acidosis results from increased levels of acid-binding to bicarbonate to produce carbon dioxide through the Henderson-Hasselbalch equation.
8.What is another name for anion gap test?
Answer : In blood test results, anion gap (also known as serum anion gap) is a measurement to check for the acid-base balance of your blood and/or an electrolyte imbalance in your blood.